
Staphylococcus aureus is a bacterium that is a member of the Firmicutes, and is frequently found in the human respiratory tract and on the skin. Although S. aureus is not always pathogenic, it is a common cause of skin infections (e.g. boils), respiratory disease (e.g. sinusitis), and food poisoning. Disease-associated strains often promote infections by producing potent protein toxins, and expressing cell-surface proteins that bind and inactivate antibodies. The emergence of antibiotic-resistant forms of pathogenic S. aureus (e.g. MRSA) is a worldwide problem in clinical medicine.
Staphylococcus was first identified in 1880 in Aberdeen, United Kingdom, by the surgeon Sir Alexander Ogston in pus from a surgical abscess in a knee joint. This name was later appended to Staphylococcus aureus by Rosenbach who was credited by the official system of nomenclature at the time. It is estimated that 20% of the human population are long-term carriers of S. aureus which can be found as part of the normal skin flora and in anterior nares of the nasal passages. S. aureus is the most common species of staphylococcus to cause Staph infections and is a successful pathogen due to a combination of nasal carriage and bacterial immuno-evasive strategies. S. aureus can cause a range of illnesses, from minor skin infections, such as pimples, impetigo, boils (furuncles), cellulitis folliculitis, carbuncles, scalded skin syndrome, and abscesses, to life-threatening diseases such as pneumonia, meningitis, osteomyelitis, endocarditis, toxic shock syndrome (TSS), bacteremia, and sepsis. Its incidence ranges from skin, soft tissue, respiratory, bone, joint, endovascular to wound infections. It is still one of the five most common causes of nosocomial infections and is often the cause of postsurgical wound infections. Each year, some 500,000 patients in American hospitals contract a staphylococcal infection.
Microbiology
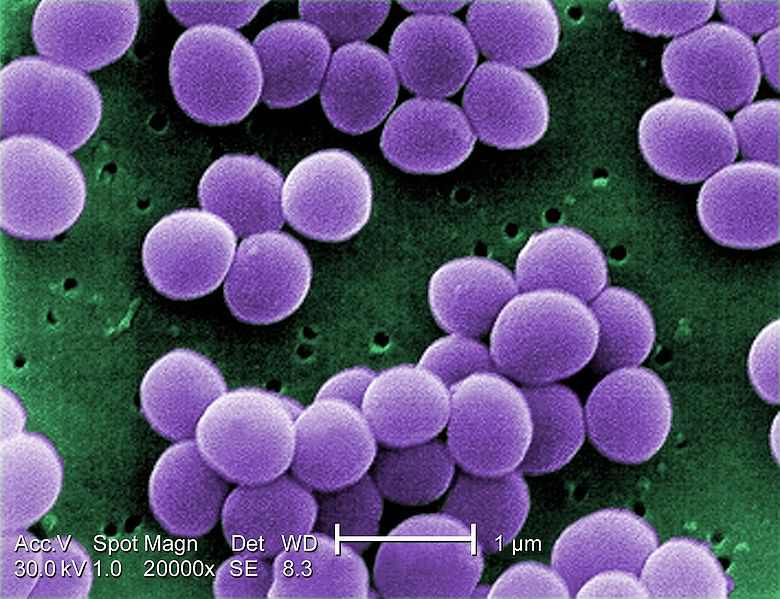
S. aureus ("grape-cluster berry", Latin aureus, "golden") is a facultative anaerobic Gram-positive coccal bacterium, also known as "golden staph" and Oro staphira. In medical literature the bacteria is often referred to as S. aureus or Staph aureus. Staphylococcus should not be confused with the similarly named and medically relevant genus Streptococcus. S. aureus appears as grape-like clusters when viewed through a microscope, and has large, round, golden-yellow colonies, often with hemolysis, when grown on blood agar plates. S. aureus reproduces asexually by binary fission. The two daughter cells do not fully separate and remain attached to one another. This is why the cells are observed in clusters.
S. aureus is catalase-positive (meaning it can produce the enzyme catalase). Catalase converts hydrogen peroxide (H2O2) to water and oxygen. Catalase-activity tests are sometimes used to distinguish staphylococci from enterococci and streptococci. Previously, S. aureus was differentiated from other staphylococci by the coagulase test. However it is now known that not all S. aureus are coagulase-positive and that incorrect species identification can impact effective treatment and control measures.
Role in disease
S. aureus is responsible for many infections but it may also occur as a commensal. The presence of S. aureus does not always indicate infection. S. aureus can survive from hours to weeks, or even months, on dry environmental surfaces, depending on strain.
S. aureus can infect tissues when the skin or mucosal barriers have been breached. This can lead to many different types of infections including furuncles and carbuncles (a collection of furuncles).
S. aureus infections can spread through contact with pus from an infected wound, skin-to-skin contact with an infected person by producing hyaluronidase that destroys tissues, and contact with objects such as towels, sheets, clothing, or athletic equipment used by an infected person. Deeply penetrating S. aureus infections can be severe. Prosthetic joints put a person at particular risk of septic arthritis, and staphylococcal endocarditis (infection of the heart valves) and pneumonia. Strains of S. aureus can host phages, such as Φ-PVL (produces Panton-Valentine leukocidin), that increase virulence.
Source: wikipedia.org
Staphylococcus was first identified in 1880 in Aberdeen, United Kingdom, by the surgeon Sir Alexander Ogston in pus from a surgical abscess in a knee joint. This name was later appended to Staphylococcus aureus by Rosenbach who was credited by the official system of nomenclature at the time. It is estimated that 20% of the human population are long-term carriers of S. aureus which can be found as part of the normal skin flora and in anterior nares of the nasal passages. S. aureus is the most common species of staphylococcus to cause Staph infections and is a successful pathogen due to a combination of nasal carriage and bacterial immuno-evasive strategies. S. aureus can cause a range of illnesses, from minor skin infections, such as pimples, impetigo, boils (furuncles), cellulitis folliculitis, carbuncles, scalded skin syndrome, and abscesses, to life-threatening diseases such as pneumonia, meningitis, osteomyelitis, endocarditis, toxic shock syndrome (TSS), bacteremia, and sepsis. Its incidence ranges from skin, soft tissue, respiratory, bone, joint, endovascular to wound infections. It is still one of the five most common causes of nosocomial infections and is often the cause of postsurgical wound infections. Each year, some 500,000 patients in American hospitals contract a staphylococcal infection.
Microbiology
S. aureus ("grape-cluster berry", Latin aureus, "golden") is a facultative anaerobic Gram-positive coccal bacterium, also known as "golden staph" and Oro staphira. In medical literature the bacteria is often referred to as S. aureus or Staph aureus. Staphylococcus should not be confused with the similarly named and medically relevant genus Streptococcus. S. aureus appears as grape-like clusters when viewed through a microscope, and has large, round, golden-yellow colonies, often with hemolysis, when grown on blood agar plates. S. aureus reproduces asexually by binary fission. The two daughter cells do not fully separate and remain attached to one another. This is why the cells are observed in clusters.
S. aureus is catalase-positive (meaning it can produce the enzyme catalase). Catalase converts hydrogen peroxide (H2O2) to water and oxygen. Catalase-activity tests are sometimes used to distinguish staphylococci from enterococci and streptococci. Previously, S. aureus was differentiated from other staphylococci by the coagulase test. However it is now known that not all S. aureus are coagulase-positive and that incorrect species identification can impact effective treatment and control measures.
Role in disease
S. aureus is responsible for many infections but it may also occur as a commensal. The presence of S. aureus does not always indicate infection. S. aureus can survive from hours to weeks, or even months, on dry environmental surfaces, depending on strain.
S. aureus can infect tissues when the skin or mucosal barriers have been breached. This can lead to many different types of infections including furuncles and carbuncles (a collection of furuncles).
S. aureus infections can spread through contact with pus from an infected wound, skin-to-skin contact with an infected person by producing hyaluronidase that destroys tissues, and contact with objects such as towels, sheets, clothing, or athletic equipment used by an infected person. Deeply penetrating S. aureus infections can be severe. Prosthetic joints put a person at particular risk of septic arthritis, and staphylococcal endocarditis (infection of the heart valves) and pneumonia. Strains of S. aureus can host phages, such as Φ-PVL (produces Panton-Valentine leukocidin), that increase virulence.
Source: wikipedia.org
 RSS Feed
RSS Feed
